
Contents
- What Is an Aortic Aneurysm?
- Types of Aortic Aneurysm
- Difference from Dissection
- How Common Is It?
- Symptoms
- Who Is at Risk?
- Does It Occur in Young People?
- How Is It Diagnosed?
- What Consequences Can It Cause?
- Can It Be Prevented?
- Treatment Methods
- Why Is the Aorta a "Ticking Time Bomb"? (Video)
- Selim İsbir's Clinical Notes
- Frequently Asked Questions
What Is an Aortic Aneurysm?
An aortic aneurysm is a balloon-like enlargement of the aorta — the largest artery leaving the heart — caused by weakening of the vessel wall. Once the diameter exceeds a certain limit, the risk of rupture increases, which can lead to a life-threatening sudden internal bleeding.
The term "aneurysm" refers to an abnormal enlargement of a blood vessel resulting from weakening of its wall. An aortic aneurysm is such an enlargement occurring in the aorta — the body's largest artery, which carries oxygen-rich blood from the heart to the rest of the body. The normal diameter of the aorta varies by region; however, once it exceeds a certain level, the risk of wall rupture increases and this can cause life-threatening sudden bleeding.
Types of Aortic Aneurysm
Aortic aneurysms are classified into four main types according to the location of the enlargement:
Ascending Aortic Aneurysm
Occurs in the first segment of the aorta leaving the heart. Usually associated with congenital valve disease or connective tissue disorders.
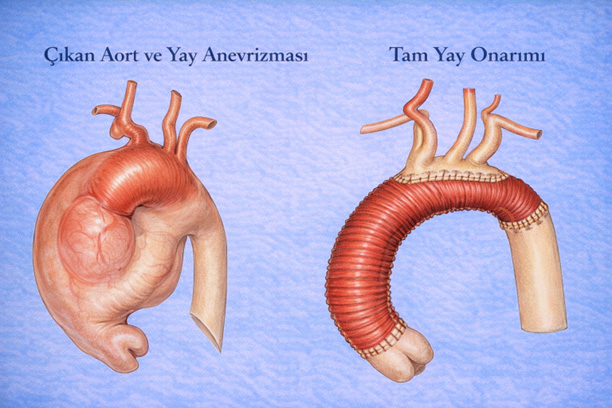
Learn more →Aortic Arch Aneurysm
Occurs in the region where the branches to the brain arise. Treatment may require the hybrid method.
Learn more →Thoracic Aortic Aneurysm
Develops in the part of the aorta within the chest cavity. Symptoms are usually hoarseness or difficulty swallowing.
Learn more →Abdominal Aortic Aneurysm
Occurs in the abdominal part of the aorta and is the most common type. Closed treatment with EVAR is possible.
Learn more →
What Is the Difference from Dissection?
Another condition that should not be confused with an aneurysm is aortic dissection. Dissection occurs when a tear forms in the inner layer of the aortic wall and blood travels between the wall layers, forming a false channel. Aneurysm and dissection can sometimes occur together. In both cases, the greatest danger is rupture of the vessel wall.
How Common Is It?
Aortic aneurysms usually run a silent course; they give no symptoms for a long time. For this reason they are most often discovered incidentally during tests performed for a different health problem. In people over 50, the frequency is about 25 per 100,000, and in Türkiye approximately 3,000–4,000 new aortic aneurysm cases are diagnosed each year.
What Are the Symptoms?
Aortic aneurysms most often cause no symptoms. However, depending on their size and location, they may sometimes lead to the following:
- Chest, back or abdominal pain
- Pulsating sensation in the abdomen (especially in thin individuals)
- Hoarseness in large aneurysms in the chest region (pressure on the vocal cords)
- Difficulty swallowing when there is pressure on the esophagus
- Sudden severe pain — may be a sign of rupture
Who Is at Risk?
The main factors that increase the risk of developing an aortic aneurysm are:
- A family history of aortic aneurysm
- A history of brain aneurysm
- Being over 70 years of age
- High blood pressure (hypertension)
- Long-term smoking
- A congenital bicuspid aortic valve
Does It Occur in Young People?
Although aortic aneurysms are usually seen at older ages, they can also occur in young people in certain special situations:
- Connective tissue disorders such as Marfan Syndrome, Loeys-Dietz Syndrome and Ehlers-Danlos Syndrome
- Congenital valve anomalies such as a bicuspid aortic valve
- Family members with a history of aortic rupture at a young age
- Genetic predisposition and connective tissue weakness
How Is an Aortic Aneurysm Diagnosed?
An aortic aneurysm is most often diagnosed with imaging methods: ultrasonography for the abdomen, echocardiography for the heart and ascending aorta, and CT angiography — the gold standard — for detailed assessment. For repeated follow-ups, MR angiography may be preferred to reduce radiation exposure.
Diagnosis begins above all with suspicion; once there is suspicion, it is clarified with imaging. The most commonly used methods are:
- Echocardiography: for assessing the heart and the ascending aorta
- Ultrasonography: for the abdominal region (abdominal aorta screening)
- CT Angiography: the gold standard for detailed assessment of the thoracic and abdominal aorta
- MR Angiography: to avoid radiation in repeated follow-ups
What Consequences Can an Aortic Aneurysm Cause?
The greatest danger of an aortic aneurysm is the risk of rupture, which arises once the vessel diameter reaches a certain point. This can cause sudden and rapidly progressing internal bleeding. Survival after rupture is very low.
Can an Aortic Aneurysm Be Prevented?
An aortic aneurysm cannot be fully prevented, but the likelihood of developing one can be reduced by controlling certain risk factors. Two factors are particularly decisive:
- Smoking: weakens the aortic wall and increases aneurysm risk. Quitting is the most effective preventive measure.
- Hypertension: by increasing pressure on the vessel wall, it accelerates the enlargement process. Target blood pressure: <130/80 mmHg.
Managing these factors can reduce the risk considerably. However, genetic factors (such as Marfan Syndrome) cannot be changed. For this reason, regular follow-up and appropriate screening are vital for individuals with a family history.
Aortic Aneurysm Treatment Methods
An aortic aneurysm is treated with three methods: open surgery (replacing the enlarged vessel with an artificial graft), the endovascular method (EVAR/TEVAR — placing a stent-graft through the groin) and the hybrid method. Which method is used is determined by the location and size of the aneurysm and the patient's general health.
The treatment approach is determined by the location, size of the aneurysm and the patient's general health. The decision is made through a joint assessment by the cardiology and cardiovascular surgery team.
Open Surgery
The breastbone is opened, the heart is stopped, the enlarged vessel is removed and replaced with an artificial graft.
Endovascular (EVAR/TEVAR)
A stent-graft is placed inside the vessel through the groin. Discharge within 1–2 days is possible.
Hybrid Method
A combination of open and closed surgery. For complex aneurysms, performed in a dedicated hybrid operating room.
1. Open Surgery
It is preferred especially for aneurysms in the segment of the aorta leaving the heart (ascending aorta and arch). In this method the breastbone (sternum) is opened; the heart is connected to a heart-lung machine and temporarily stopped, and the enlarged segment of the vessel is removed and replaced with an artificial graft.
- Advantage: in young patients in good general condition, long-term durability and outcomes are good.
- Disadvantage: the recovery period is longer than with the closed method (3–4 weeks).
- Hospital stay: usually 5–6 days.
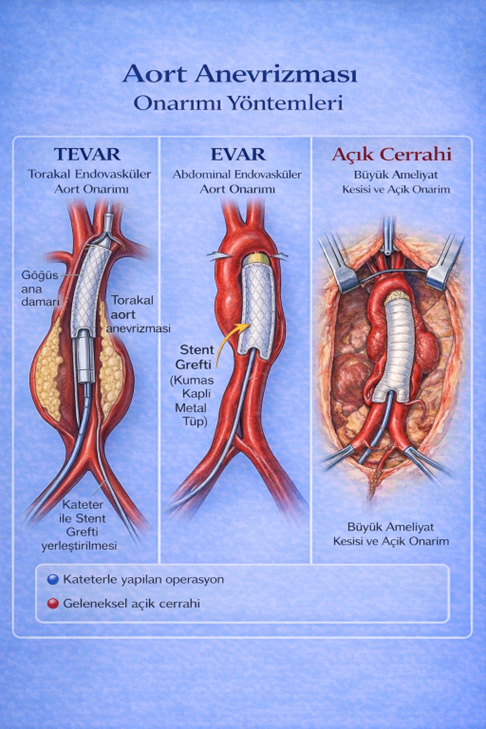
2. Endovascular Method (EVAR/TEVAR)
It is suitable especially for abdominal aortic aneurysms and some thoracic aneurysms. The procedure is performed through a small incision in the groin; a special stent-graft is placed inside the vessel and the enlarged segment is disabled from within.
- Intensive care and hospital stay are usually shorter (1–2 days).
- The risk of infection and blood loss is lower.
- The return to normal life is much faster.
- EVAR: for the abdominal region
- TEVAR: for the thoracic region
3. Hybrid Method
For complex aneurysms that also involve the vessels supplying the brain, a combination of open and closed surgery is used. Most often, a bypass to the brain vessels is performed without stopping the heart; then an endovascular graft is placed to disable the enlarged segment. This approach should be performed in hybrid operating rooms with advanced imaging and surgical infrastructure.
Related Videos
In an interview, Prof. Dr. Selim İsbir explains why an aortic aneurysm is so insidious and what rupture means (translated from Turkish):
— The aorta is our largest vessel. Can it really turn into a "ticking time bomb" for the body?
"Absolutely. The worst thing about aortic aneurysms is that they are very insidious diseases."
— So it gives no symptoms?
"It gives no symptoms. Here's why: both the chest cavity and the abdominal cavity are very spacious. So the aorta can grow here silently."
— And if no intervention is made in an aortic aneurysm?
"At the moment it ruptures, the mortality risk is about 50%. Roughly half of patients die at the very moment of rupture. Those who are lucky — if they are close to a healthcare facility or to a place where heart surgery is performed — must be taken to surgery immediately, on a very urgent basis, without losing any time."
— Prof. Dr. Selim İsbir, Cardiovascular Surgery
What Is an Aneurysm, What Is an Aortic Aneurysm?
An aneurysm is a balloon-like enlargement of a vessel wall caused by its weakening. It is most often seen in the aorta, the main vessel leaving the heart. If enlargement occurs anywhere along this vessel, it is called an aortic aneurysm.
3 Aneurysm Zones — A Simple Explanation
In addition to the 4-type medical classification above, I prefer to explain aneurysms to my patients roughly by 3 zones:
- Thoracic (chest region): the part of the main vessel leaving the heart that is inside the chest. Symptom: chest or back pain.
- Abdominal (abdominal region): the part of the aorta inside the abdomen. The most common type. Symptom: pulsating sensation in the abdomen, lower back/abdominal pain.
- Thoracoabdominal (both): involves both the chest and abdominal parts together. It affects a wider area and its treatment is more complex.
Symptoms — Most Patients Have None
The most insidious aspect of an aortic aneurysm is that in most patients it gives no symptoms at all. It can grow for years without being noticed. If it does give symptoms:
- Chest, back or abdominal pain
- A pulsating sensation in the abdomen
- Sudden severe pain — in this case call 112 immediately (suspected rupture)
For this reason, if you are in the risk group (age, smoking, blood pressure, family history) — you must get screened without waiting for symptoms.
When Is Surgery Needed?
The decision to operate is not made on a single criterion. Surgery is planned if one of the following is present:
- The aneurysm diameter reaches 4.5–5 cm or more
- It shows rapid growth (more than 5 mm per year)
- It causes pain or other complaints
- The rupture risk is high
- Rupture has occurred — emergency surgery
Aneurysms below this threshold are kept under follow-up: blood pressure control and regular imaging.
Treatment and Recovery Time — Open vs Closed
This is the question my patients ask most — "how long will I stay in hospital, when can I return to work?"
- Open surgery: 5–6 days in hospital. Return to normal life in 3–4 weeks. A lasting solution in the long term.
- Closed method (EVAR/TEVAR): 1–2 days in hospital. A much faster return to normal life. However, it is not suitable for every patient.
To find out whether the closed method is suitable for you, a detailed CT angiography is needed. The anatomy and diameter of the vessels and the health of the zones where the stent will sit determine success.
It Progresses Silently — Regular Check-ups Save Lives
If there is one thing you should know about an aortic aneurysm, it is this: it gives no symptoms, grows silently, and when it ruptures it may be too late. If you are in the risk group (50+ years, male, smoking, hypertension, family history) — having an abdominal ultrasound once a year, and echocardiography when needed, can save your life.
Scientific Sources
- European Society for Vascular Surgery (ESVS): Clinical Practice Guidelines on Abdominal Aorto-iliac Artery Aneurysms
- ACC/AHA 2022: Guideline for the Diagnosis and Management of Aortic Disease
- Mayo Clinic: Aortic Aneurysm — Symptoms and Causes
- European Society of Cardiology (ESC): Guidelines on the Diagnosis and Treatment of Aortic Diseases
Frequently Asked Questions
Book an Appointment
Prof. Dr. Selim İsbir — Yeditepe University Koşuyolu Hospital