
What is the Pericardium and What are its Functions?
The pericardium is a double-layered, sac-like structure that surrounds the heart. It consists of two layers: an inner (visceral) and an outer (parietal) layer. Between these two layers, there is a small amount (approximately 15-50 ml) of pericardial fluid that minimizes friction during the heart’s contraction and relaxation. The primary functions of the pericardium include:
- Protecting the heart from infections and trauma that may originate from neighboring organs.
- Stabilizing the heart’s position by preventing its excessive expansion (acute dilation).
- Contributing to the pressure balance between the heart chambers.
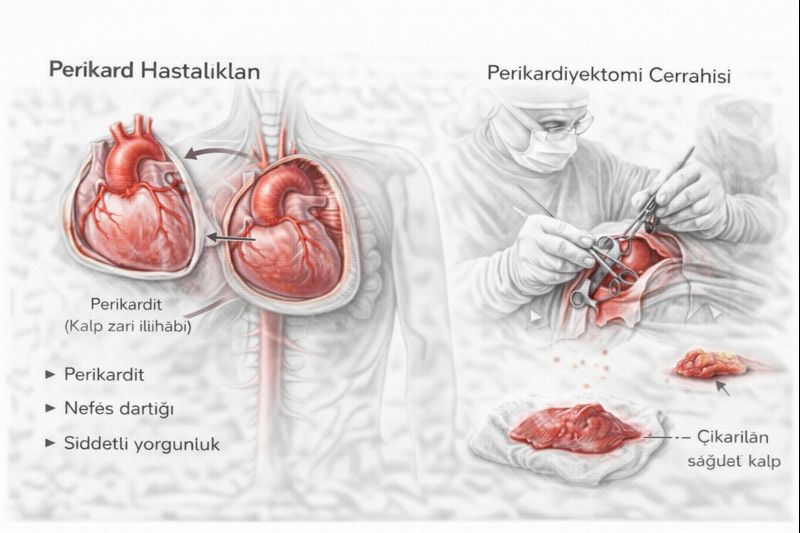
Common Pericardial Diseases
- Acute Pericarditis: Sudden inflammation of the pericardial layers. It usually develops after viral infections and causes sharp, stabbing chest pain.
- Pericardial Effusion: Accumulation of more fluid than normal between the pericardial layers. If the fluid volume increases slowly, the heart can adapt, but rapid accumulation (cardiac tamponade) is life-threatening.
- Cardiac Tamponade: Pericardial effusion creating enough pressure to impede the filling of the heart chambers. It is a critical condition requiring emergency intervention, which can lead to shock and cardiac arrest.
- Constrictive Pericarditis: Thickening, hardening, and calcification of the pericardium after chronic inflammation or injury. This “armor-like” structure severely restricts the heart’s relaxation (diastolic) phase, leading to symptoms of right heart failure.
What Causes Pericardial Diseases? Risk Factors
The underlying causes of pericardial diseases vary:
- Idiopathic (Unknown Cause): A clear cause cannot be found in most cases, especially acute pericarditis.
- Infections: Viral (Coxsackie, influenza), bacterial (tuberculosis), or fungal infections.
- Cardiac Surgery or Trauma: After heart surgeries (postpericardiotomy syndrome) or blows to the chest.
- Radiation Therapy: Can develop years after radiotherapy, especially when applied to the chest area.
- Autoimmune Diseases: Systemic inflammatory diseases such as lupus, rheumatoid arthritis.
- Cancer: Spread (metastasis) of cancers such as lung, breast cancer, or lymphoma to the pericardium.
- Kidney Failure (Uremia): Elevated urea levels in the blood can irritate the pericardium.
Symptoms: Signs of Pressure on the Heart
Symptoms vary depending on the type and severity of the underlying pericardial disease:
- Chest Pain: A typical symptom of acute pericarditis. It is usually a sharp, stabbing pain that radiates to the back and decreases when leaning forward.
- Shortness of Breath: The most common symptom, especially in constrictive pericarditis. It increases with exertion due to the heart’s inability to pump enough blood.
- Swelling in Legs and Abdomen (Edema/Ascites): A sign of fluid accumulation in the body, and an advanced symptom of constrictive pericarditis and heart failure.
- Fatigue and Weakness: A general symptom due to insufficient blood being pumped to the body.
- Palpitations and Irregular Heartbeat: Can be seen as a result of pressure on the heart or inflammation spreading to the heart muscle.
How are Pericardial Diseases Diagnosed?
Patient history and physical examination findings are crucial for accurate diagnosis. The physician may hear a “pericardial friction rub” with a stethoscope. The following tests are used to confirm the diagnosis:
- Echocardiography (ECHO): The primary method for evaluating pericardial fluid, membrane thickness, and heart contraction and relaxation functions.
- Electrocardiogram (ECG): Can show typical changes specific to acute pericarditis.
- Chest X-ray: Can show the size of the heart shadow (cardiomegaly) and calcification in the pericardium.
- Computed Tomography (CT) and Magnetic Resonance Imaging (MRI): Show the thickness, calcification, and relationship of the pericardium with surrounding tissues in great detail. It is particularly critical for surgical planning.
- Cardiac Catheterization: Directly measures pressures within the heart chambers, revealing hemodynamic evidence of constrictive pericarditis and confirming the diagnosis.
Pericardiectomy Surgery: The Surgery That Frees the Heart
Pericardiectomy is the surgical removal of the thickened, hardened pericardial membrane that restricts heart movement, to the greatest extent possible. This surgery is the only treatment method that provides a permanent cure, especially for chronic constrictive pericarditis. The goal is to remove the mechanical barrier in front of the heart, allowing the chambers to fill freely and pump blood effectively.
When is Surgery Decided?
The decision for pericardiectomy is made with a multidisciplinary approach based on the patient’s symptoms, disease severity, and underlying cause:
- Chronic Constrictive Pericarditis: The most important indication for patients with significant heart failure symptoms and a confirmed diagnosis.
- Recurrent Pericardial Effusion: Conditions requiring frequent hospitalizations or impairing quality of life due to continuous fluid accumulation.
- Calcific Pericarditis: Cases where the pericardium is heavily calcified and encases the heart like armor.
- Constriction Developing After Radiation or Surgery: Cases unresponsive to other treatments.
How is the Surgery Performed? (Step-by-Step)
- Access: The surgery is usually performed by cutting the breastbone down the middle (median sternotomy). This provides the widest and safest access to the heart.
- Preparation: After exposing the heart and major vessels, the surgeon prepares for connection to a heart-lung machine (cardiopulmonary bypass) if necessary. However, many experienced centers prefer to perform this surgery on a beating heart.
- Pericardial Dissection: This is the most critical and delicate stage of the surgery. The surgeon carefully separates the thickened pericardial layer, which is adhered to the heart, from the heart muscle (myocardium). Great care is taken to avoid damaging the coronary arteries that supply the heart and the thin-walled right ventricle.
- Release: The goal is to remove all constricting tissue around the anterior and diaphragmatic surfaces of the heart and the major vessels. This ensures the complete release of both the right and left sides of the heart.
- Control and Closure: After the removal process is complete, bleeding control is performed, drains are placed, and the breastbone is closed, concluding the surgery.
Potential Risks and Complications
Although pericardiectomy has a high success rate in experienced hands, it involves serious risks:
- Bleeding: There is a high risk of bleeding in areas where the pericardium is adhered to the heart.
- Low Cardiac Output Syndrome: The heart muscle, which has been under prolonged pressure, struggles to adapt to sudden release after surgery. It may require medication support in intensive care.
- Heart Muscle or Coronary Artery Injury: A serious complication that can occur during dissection.
- Arrhythmias (Rhythm Disorders): Can be common after surgery and are usually temporary.
Post-Surgery Recovery and Follow-up
Patients are monitored in intensive care for a few days after surgery. During this period, fluid balance and heart functions are closely observed. Expected outcomes after successful surgery include:
- Rapid Symptomatic Improvement: Significant reduction in shortness of breath and edema.
- Hemodynamic Improvement: Normalization of intracardiac pressures.
- Long-Term Follow-up: Regular follow-up with echocardiography and clinical examination is important to ensure full recovery of heart functions.
Other Treatment Methods
Non-surgical treatments are prioritized, especially in acute pericarditis and uncomplicated effusions:
- Medication Therapy: Anti-inflammatory drugs (aspirin, ibuprofen), colchicine, and corticosteroids are used in the treatment of acute pericarditis.
- Pericardiocentesis: The procedure of draining fluid from the pericardial space with a needle, for cardiac tamponade or diagnostic purposes.
Lifestyle and Long-Term Management
It is important for individuals diagnosed with pericardial disease to restrict salt intake, regulate fluid intake under medical supervision, and adhere to regular check-ups. The level of physical activity should be determined by the physician based on the stage of the disease.
Conclusion
Pericardial diseases span a wide spectrum, ranging from simple inflammation to life-threatening cardiac compression. Constrictive pericarditis, in particular, is an insidious condition that mechanically chokes the heart and leads to progressive heart failure. For these patients, Pericardiectomy is the gold standard treatment method that frees the heart from its armor, restoring normal function and improving quality of life and survival. Pericardial diseases should always be considered and evaluated by a multidisciplinary team in patients with unexplained shortness of breath, edema, and fatigue, especially those with a history of cardiac surgery or radiotherapy.