
How Do the Heart and Mitral Valve Work?
Our heart is a powerful, four-chambered pump (right-left atrium and right-left ventricle) that works tirelessly throughout life. There are four main valves that ensure blood flows in the correct direction between these chambers. The mitral valve holds strategic importance among them.
It is located between the left atrium (where oxygenated blood from the lungs collects) and the left ventricle (the main chamber that pumps blood to the body). It has two leaflets and is named after its resemblance to a bishop’s miter. During the heart’s relaxation phase (diastole), it opens to allow blood to fill the ventricle; during contraction (systole), it closes completely to prevent blood from flowing backward and directs it into the aorta.
Causes of Mitral Valve Diseases
Mitral valve diseases are examined in two main groups based on their origin: genetic or acquired.
Congenital Causes and MVP
In some individuals, the valve structure is different from birth (e.g., cleft mitral valve). However, the most common and widespread condition in this group is Mitral Valve Prolapse (MVP).
Mitral Valve Prolapse: The tissue of the valve leaflets is structurally loose and flexible. When the heart contracts, the leaflets bulge like a parachute into the left atrium. This condition is sometimes harmless, but in advanced stages, the valve cannot close completely and causes severe mitral regurgitation (blood leakage). It is usually genetically inherited.
Acquired Causes
- Rheumatic Fever: This is the most common cause in developing countries like Turkey. Untreated beta-hemolytic streptococcal throat infections in childhood confuse the body’s immune system, causing it to attack the heart valves. Years later, it manifests as thickening, adhesion, and calcification (mitral stenosis) of the valves.
- Aging and Calcification: With advanced age, degenerative calcifications can occur in the valve annulus and leaflets.
- Ischemic Heart Disease (Heart Attack): After a heart attack, acute or chronic valve insufficiency can develop due to damage to the muscles or cords (chordae) that support the mitral valve.
- Endocarditis: This is an infection of the inner lining of the heart and the valves. It can perforate or damage the valve structure, requiring urgent intervention.
Types of Disease: Stenosis and Regurgitation
Mitral valve dysfunction manifests mechanically in two ways:
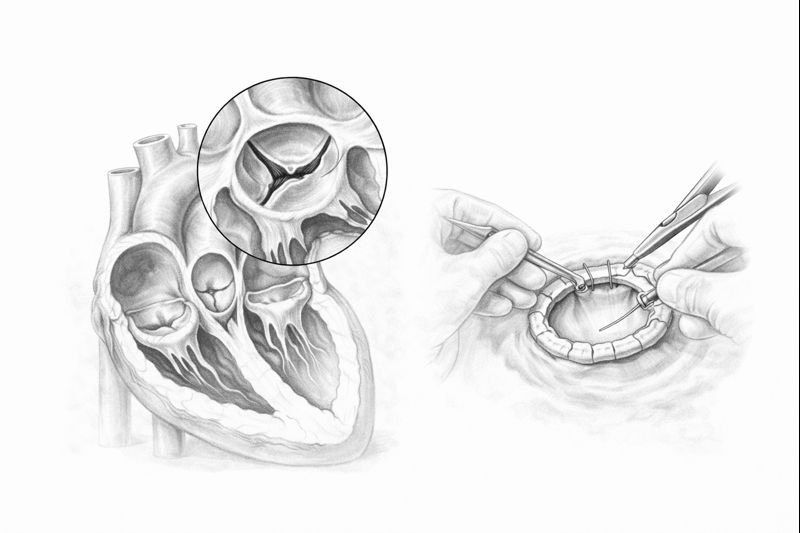
- Mitral Valve Stenosis: The valve leaflets calcify or stick together. The valve cannot open sufficiently (fish-mouth appearance). Blood struggles to pass into the left ventricle and accumulates in the left atrium. This pressure reflects backward into the lungs, causing shortness of breath.
- Mitral Valve Regurgitation: The valve cannot close completely. Each time the heart contracts, while some blood goes to the body, a significant portion leaks backward (into the left atrium). The heart has to work harder to meet the body’s needs and eventually enlarges (cardiac dilation).
The Body’s Signals: Symptoms
The disease may progress silently in its early stages. However, when the heart’s reserves are depleted, the following symptoms begin:
- Shortness of Breath: This is the most prominent symptom. Initially, it occurs with exertion (walking, stairs), but in later stages, it is seen at rest and especially when lying down at night (inability to lie flat, need to increase the number of pillows).
- Palpitations: Mitral stenosis and regurgitation enlarge the left atrium, creating a predisposition for an arrhythmia called Atrial Fibrillation.
- Easy Fatigability: Weakness is observed because insufficient oxygen is transported to the tissues.
- Hemoptysis: In severe stenoses, if lung pressure increases significantly, bloody sputum may be coughed up.
- Edema: If right heart failure is also present, swelling in the legs occurs.
Diagnostic Methods
The diagnostic process begins with an examination by a cardiology specialist. A murmur heard with a stethoscope is the first sign of valve disease.
- Echocardiography (ECHO): This is the basis of diagnosis. The structure of the valve and the degree of stenosis or leakage are clearly measured.
- Transesophageal ECHO (TEE): This procedure, performed via the esophagus, provides a very clear view, especially of the posterior aspect of the mitral valve. It is essential if a decision for surgery or repair is to be made. It is also crucial for checking for the presence of clots.
- Coronary Angiography: Performed in patients over 40 years of age before surgery to check for blockages in the coronary arteries.
Treatment Options
The treatment strategy is determined individually based on the severity of the disease, the patient’s age, and co-existing conditions.
1. Medical Treatment and Follow-up
Medications cannot correct a mechanical valve problem, but they can lighten the heart’s load. Diuretics (to reduce edema), rhythm regulators, and anticoagulant blood thinners are used. In mild cases, regular ECHO follow-up is sufficient.
2. Mitral Valve Repair (Plasty)
Today, this is the gold standard in surgery. Especially in degenerative regurgitation and MVP patients, repair is performed while preserving the patient’s own valve.
- Heart functions are better preserved.
- The risk of infection is low.
- There is no lifelong need for blood thinners after surgery.
3. Mitral Valve Replacement
If the valve is excessively calcified or too damaged to be repaired (especially in rheumatic stenoses), it is replaced with an artificial valve.
- Mechanical Valve: Very durable, lasts a lifetime, but requires continuous use of blood thinners (Coumadin/Warfarin).
- Biological Valve: Made from animal tissue. Does not require blood thinners but has a lifespan of 10-15 years. Preferred for elderly patients.
4. Minimally Invasive and Robotic Surgery
This is the greatest comfort brought by technology. Surgery is performed through small 4-5 cm incisions under the right armpit or below the breast, without cutting the breastbone (sternum). In robotic surgery, the surgeon controls the arms from a console.
- Less pain and bleeding occur.
- Recovery time is much faster.
- Cosmetic results are excellent; no large surgical scar remains.
5. Non-Surgical Method: MitraClip
Applied to patients with a very high risk for open-heart surgery (advanced age, kidney failure, etc.). By entering through the groin like an angioplasty, the two leaking leaflets of the mitral valve are clipped together with a “clip.” This reduces the leakage, and the patient is discharged in a short time.
What Happens If Left Untreated?
Mitral valve diseases are a mechanical problem and progress over time. If left untreated:
- Heart Failure: The heart muscle irreversibly weakens.
- Pulmonary Hypertension: Lung vascular pressure increases.
- Stroke: A clot formed in the left atrium can travel to the brain.
Early diagnosis saves lives. If you experience shortness of breath or palpitations, it is vital to consult a cardiology specialist and have your heart checked with a simple echocardiogram.