
Coronary Arteries and Their Functions
The heart is the body’s engine and works non-stop. For this intense workload, its muscle tissue (myocardium) constantly needs fresh blood, oxygen, and nutrients. The blood inside the heart cannot directly nourish the heart muscle; this task is undertaken by the coronary arteries, which wrap around the outer surface of the heart like a net.
There are two main systems:
- Left Main Coronary Artery (LMCA): Supplies the left side of the heart, which performs the main pumping function. It divides into two:
- LAD (Left Anterior Descending Artery): Supplies the front surface of the heart. Its blockage carries a vital risk (also known as the “widowmaker artery”).
- Cx (Circumflex Artery): Supplies the left side and back of the heart.
- Right Coronary Artery (RCA): Supplies the right side of the heart and the center of its electrical system.
How Does the Disease Develop? (Atherosclerosis)
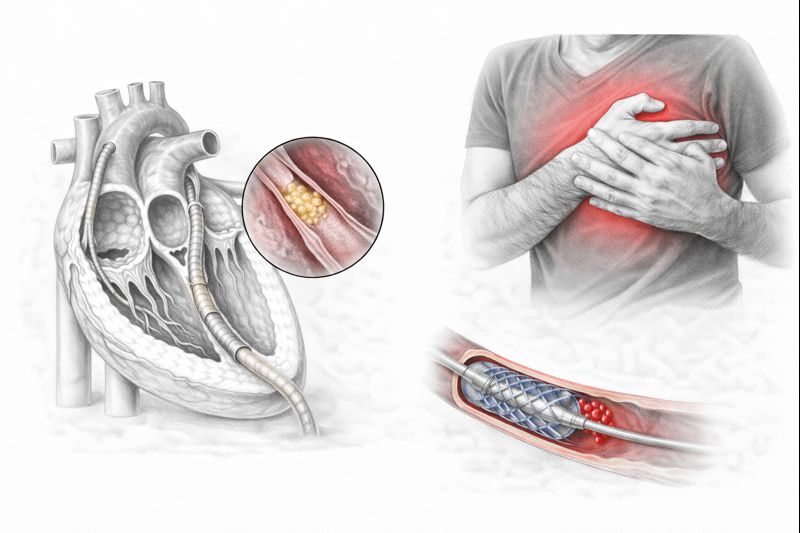
A healthy coronary artery has a smooth interior and free blood flow. However, over time, due to high cholesterol in the blood, cigarette toxins, and high blood pressure, the inner wall of the vessel is damaged. As the body tries to repair this damage, inflammatory cells and fats (cholesterol) accumulate in the area. This is called atherosclerosis (hardening of the arteries).
These accumulated structures eventually calcify, forming mounds we call “plaques.” As plaques grow, they narrow the inside of the vessel. When a critical threshold is exceeded, two scenarios occur:
- Stable Angina: The plaque grows slowly, and the patient only experiences chest pain when exerting themselves (walking, climbing stairs).
- Heart Attack (Acute Syndrome): Plaque suddenly ruptures. Blood cells rushing to the ruptured area form a clot within seconds, completely blocking the vessel. The heart muscle cannot be nourished and dies. This is an emergency.
Risk Factors
CAD develops from a combination of genetic predisposition and lifestyle. Knowing the risks is the first step in prevention.
Non-Modifiable Factors
- Age: Our blood vessels age with us. The risk increases for men over 45 and women over 55.
- Gender: It is more common and occurs at an earlier age in men. In women, the risk equalizes with men after menopause due to the loss of estrogen protection.
- Family History: The risk is high if there is a history of heart attack or sudden death at a young age (under 55 for men, under 65 for women) in first-degree relatives (mother, father, sibling).
Modifiable Factors
- Smoking: This is the most important factor that damages the inner structure of blood vessels and increases clotting.
- High Blood Pressure (Hypertension): Pressurized blood flow damages vessel walls.
- High Cholesterol: Especially high LDL (bad cholesterol) and low HDL (good cholesterol).
- Diabetes (Sugar Disease): Considered a “silent heart disease.” The vascular structure of diabetics deteriorates more quickly.
- Obesity and Inactivity: Negatively affects the entire metabolism.
- Stress: Chronic stress triggers inflammation and high blood pressure in the body.
The Body’s Signals: Symptoms
The disease can remain “silent” until the vascular narrowing reaches a certain level (around 70%). When symptoms begin, the most typical sign is chest pain.
- Angina Pectoris (Chest Pain): Typically described as pressure, tightness, burning, or a heavy sensation behind the breastbone. It can spread to the left arm, neck, jaw, or back.
- Characteristic: Worsens with exertion, stress, or cold weather; subsides within 5-10 minutes with rest or sublingual medication.
- Shortness of Breath: Getting tired and out of breath more quickly than your peers during exertion.
- Heart Attack Symptoms: Severe chest pain, starting suddenly at rest, lasting longer than 20 minutes, feeling like “an elephant sitting on the chest.” Accompanied by cold sweats, fear of death, and nausea. Emergency services (112) should be called.
Diagnostic Methods
Early diagnosis saves lives. Your cardiologist may use the following tests:
- ECG (Electrocardiography): Measures the electrical activity of the heart. It is very valuable during a heart attack or in detecting traces of a past attack.
- Stress Test (Treadmill): Shows whether there is a nutritional disorder (ischemia) when the heart’s workload is increased.
- Echocardiography (ECHO): Heart ultrasound. Shows the contractile strength of the heart walls and the condition of the valves.
- CT Angiography (Virtual Angiography): Imaging of blood vessels using a tomography device. Used for screening in low-to-moderate risk patients.
- Coronary Angiography (Classic Angiography): The gold standard in diagnosis. A contrast agent is injected into the heart via a vein in the groin or wrist, and narrowings are visualized millimeter by millimeter. It allows for treatment (stent) in the same session.
Treatment Methods
Treatment is determined by the “Cardiology and Cardiovascular Surgery Council” based on the structure of the vessels, the degree of narrowing, and the patient’s general condition.
1. Medical Treatment
For mild narrowings or for protection after an interventional procedure.
- Blood Thinners: (Aspirin, etc.) Prevent clot formation.
- Statins: Lower cholesterol and stabilize plaque (prevent rupture).
- Beta-Blockers: Slow down the heart rate, reducing oxygen demand.
2. Balloon and Stent (Interventional Procedures)
Performed in the cath lab for suitable narrowings.
- Balloon Angioplasty: A deflated balloon is advanced to the narrowed area and inflated to open the vessel.
- Stent: A metal mesh placed to prevent the re-narrowing of the area opened by the balloon. Today, drug-eluting stents are commonly used; these stents release drugs that prevent tissue regrowth.
3. Bypass Surgery (CABG)
Surgery is preferred if there are narrowings in many vessels, if the main vessel is blocked, or if the patient is diabetic. Vessels taken from another part of the body (leg vein or chest artery) are sewn beyond the blocked area to create a new “bridge” (bypass).
- Importance: Can offer a more long-term and definitive solution compared to stenting. Especially when an artery taken from inside the chest (IMA) is used, the patency rate is very high.
Prevention and Lifestyle
In CAD treatment, even if a stent is placed or surgery is performed, the disease is not considered completely “over.” Atherosclerosis is a systemic process. To prevent recurrence:
- Mediterranean Diet: Eat a diet rich in olive oil, fish, vegetables, fruits, and whole grains. Avoid solid fats and processed foods.
- Quit Smoking: The risk of heart attack decreases by 50% one year after quitting smoking.
- Be Active: Walk briskly for at least 150 minutes a week.
- Monitor Your Values: Keep your blood pressure, blood sugar, and cholesterol levels within the target ranges recommended by your doctor.
Video
Coronary Artery Disease – Expert Opinion
Most Frequently Asked Questions About Coronary Artery Disease
► Does coronary artery disease completely heal?
The disease does not completely disappear, but it can be controlled. Even if the vessel is opened with a stent or bypass, the process of atherosclerosis can continue. Therefore, lifestyle changes and medication are important for life.
► Is a stent or bypass better?
This decision is made based on the patient’s condition. If there are short narrowings in one or two vessels, a stent is preferred. However, if there are blockages in many vessels, main vessel disease, or diabetes, bypass surgery offers a more lasting and healthier solution in the long term.
► Can coronary artery blockage progress without symptoms?
Yes, the disease can progress without symptoms, known as “silent ischemia.” Especially in diabetic patients, the risk of heart attack is higher due to reduced pain sensation. Regular check-ups are therefore vital.
► Is angiography dangerous?
Coronary angiography is a procedure with very low risk (less than 1 in 1000) when performed by experts. It is the gold standard method for diagnosis and, if necessary, intervention in the same session.
► I have a family history of heart disease, what should I do?
Genetic factors increase risk. Those with a family history of early heart attack should undergo regular cardiological check-ups from their 30s and closely monitor their cholesterol and blood pressure levels.
Do You Have More Questions?
We have compiled the 25 most frequently asked questions and expert answers from our patients, covering everything from heart attack symptoms to nutrition recommendations, life after stenting, and sexual health, in our special guide.