
In a small percentage of patients who experience acute pulmonary embolism (blood clot), the body cannot completely dissolve the clot. Over time, these clots adhere to the vessel wall, harden, transform into a type of “scar tissue,” and obstruct the vessel. This condition increases pulmonary pressure. In this guide, you will find every detail, from the insidious “honeymoon period” to the intricacies of PTE surgery, performed in only a few centers worldwide.
[Image of pulmonary circulation system]
What is CTEPH? How Do Clots Calcify?
Under normal circumstances, when a clot travels to the lung, the body dissolves it within 3-6 months with blood thinners. However, in CTEPH patients, this process fails. Instead of dissolving, the clot turns into a hard tissue called fibrosis, integrates with the vessel wall, and forms “web”-like structures or complete blockages that narrow the vessel.
This mechanical obstruction makes it difficult for the right heart to pump blood to the lungs. The heart is forced to work under higher pressure (Pulmonary Hypertension) and eventually tires, leading to right heart failure.
Why Did It Happen to Me? Risk Factors
Not everyone who experiences an embolism develops CTEPH. The risk factors predisposing to this disease are:
- Recurrent Embolisms: A history of multiple blood clots.
- Large Clot Burden: The initial embolic attack being very severe and widespread.
- Splenectomy: Removal of the spleen (can affect blood cell structure and increase clotting).
- History of Cancer: Blood is more prone to clotting in cancer patients.
- Chronic Diseases: Inflammatory bowel diseases or thyroid medication use.
- Blood Type: Individuals with blood types A, B, or AB have a slightly higher risk compared to type O.
The Insidious Danger: The “Honeymoon Period” and Symptoms
The most misleading aspect of CTEPH is the “Honeymoon Period.” A patient who has had an acute embolism feels better with treatment and may have no symptoms for several months or years. However, the vessels inside continue to slowly become obstructed. By the time symptoms reappear, the disease may have progressed:
- Dyspnea on Exertion: The earliest and most common symptom. Shortness of breath when walking or climbing stairs.
- Palpitations and Chest Pain: Signs of the heart being strained.
- Leg Swelling (Edema): Occurs when right heart failure begins.
- Fainting (Syncope): Occurs in advanced stages due to reduced blood flow to the brain.
Diagnostic Methods: V/Q Scintigraphy
If a patient with shortness of breath is treated for asthma or COPD but does not improve, CTEPH should be considered. The most critical diagnostic tests are:
- V/Q Scintigraphy (Ventilation/Perfusion): The gold standard for CTEPH screening. It shows the mismatch between lung ventilation and perfusion.
- Echocardiography (ECHO): Measures right heart enlargement and pulmonary pressure.
- Right Heart Catheterization: Essential for definitive pressure measurement and surgical decision-making.
- Pulmonary Angiography: Shows whether the obstruction is surgically accessible.
Treatment Options
Among the types of “Pulmonary Hypertension,” CTEPH is the only type with a chance of cure (complete recovery). The treatment decision is made by a council consisting of pulmonologists, cardiologists, and cardiac surgeons.
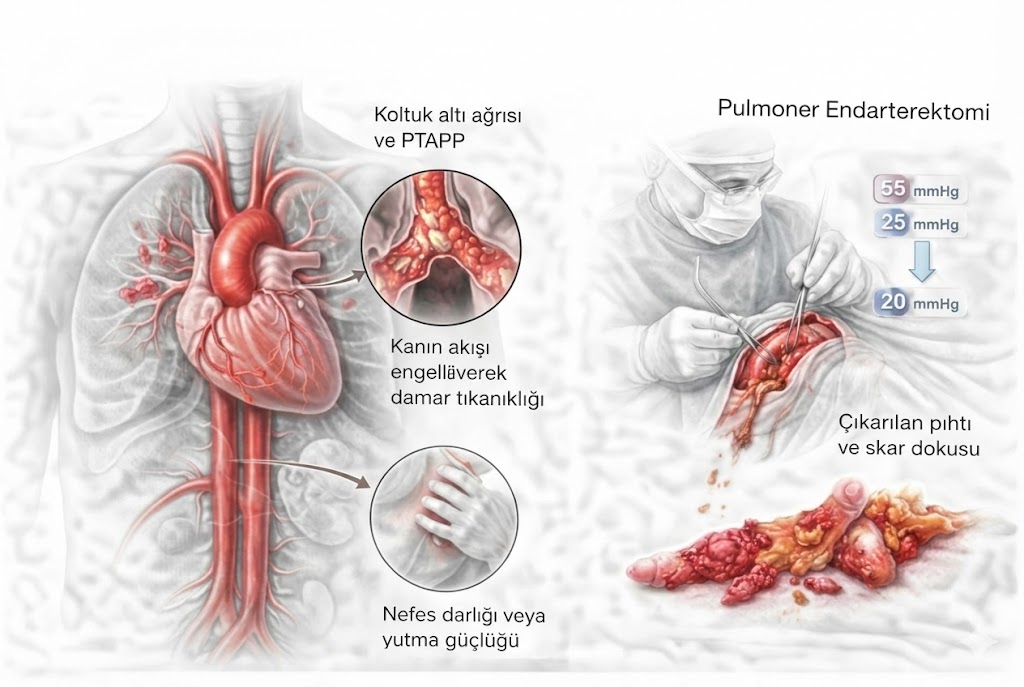
1. Gold Standard: Pulmonary Thromboendarterectomy (PTE)
This surgery is not a simple clot removal procedure. The inner wall of the vessel (intima), along with the adherent clot layer, is meticulously peeled away like “peeling an orange,” as a thin membrane.
- How is it done? The chest cavity is opened. Due to the precision required, the body temperature is cooled to 20 degrees, and the heart-lung machine is stopped (circulatory arrest) to clean the vessel with microscopic precision in a bloodless field.
- Result: After a successful PTE, pulmonary pressure returns to normal, and the patient can achieve a healthy life without medication.
2. Balloon Pulmonary Angioplasty (BPA)
Applied when clots are in distal branches too small for surgery or if the patient cannot tolerate surgery. In the angio unit, narrowings within the vessels are widened with a balloon. Typically, 4-6 sessions are required.
3. Medical Treatment
For patients unsuitable for surgery or balloon angioplasty, or to reduce residual hypertension after a procedure, specific pulmonary hypertension medications (e.g., Riociguat) are used. Additionally, all patients must take blood thinners for life.
Life After Surgery
PTE surgery is a challenging process, but the reward is significant. After the recovery period, in the vast majority of patients:
- Shortness of breath completely disappears.
- Right heart failure regresses, and the heart shrinks.
- The need for oxygen support is eliminated.
- Normal exercise capacity is restored.
Frequently Asked Questions (FAQ)
How risky is CTEPH surgery?
PTE (Pulmonary Thromboendarterectomy) is a complex surgery requiring high expertise. In experienced centers (performing above a certain number of cases per year), the surgical risk is around 2-5%. Considering the fatal course of the disease if left untreated, this risk is within acceptable limits.
Don’t blood thinners dissolve the clot?
No. The clot in CTEPH is not fresh; it is organized, hard tissue (scar tissue). Blood thinners only prevent new clot formation; they cannot open existing hardened obstructions. Mechanical cleaning (surgery or balloon) is essential.
Can clots recur after surgery?
Areas cleared by surgery generally remain open. However, it is vital for the patient to take blood thinners for life to prevent recurrence of the disease. There is a risk of relapse if medications are used irregularly.
Can I fully recover?
Yes. CTEPH is the only type of pulmonary hypertension for which a “cure” (complete healing) can be achieved. After successful surgery, patients often stop pulmonary hypertension medications and return to their normal lives.
