

In this comprehensive guide, we cover in detail how this silent danger in the chest develops, its warning signs such as back pain, the differences between open surgery and the modern TEVAR (Endovascular Stent Graft) method, and the treatment process.
Anatomy: Where is the Thoracic Aorta?
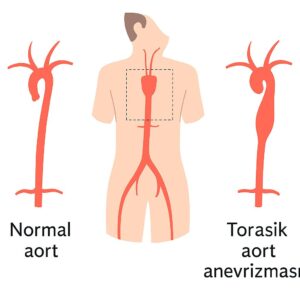
The aorta is shaped like a cane. It exits the heart, forms an arch, and descends behind the rib cage (to the left of the spine). The thoracic aorta is this “descending” part, which begins after the arch region and extends to the diaphragm.
[Image of thoracic aorta anatomy]
This region is surgically very sensitive due to being the origin of the small vessels that supply the spinal cord.
What Causes Them? Risk Factors
Thoracic aneurysms usually occur as a result of structural weakening of the vessel wall. The most common causes are:
- Atherosclerosis (Hardening of the Arteries): Plaques form in the vessel wall due to smoking, high cholesterol, and advanced age. These plaques weaken the vessel wall, creating a predisposition to enlargement.
- Hypertension: Uncontrolled high blood pressure constantly hits the vessel wall like a “sledgehammer,” causing it to expand.
- Genetic Diseases: Connective tissue diseases such as Marfan Syndrome, Loeys-Dietz, and Ehlers-Danlos syndrome are the most important causes of aneurysm formation at a young age.
- Trauma: Chest traumas such as severe traffic accidents or falls from a height can lead to injury (traumatic transection) in this region of the aorta.
The Body’s Signals: Symptoms
Aneurysms usually grow silently. However, as their diameter increases (typically above 5-6 cm), they cause symptoms by pressing on adjacent organs:
- Back Pain: This is the most common symptom. A continuous, dull, and piercing pain may be felt between the shoulder blades.
- Hoarseness: Occurs when the expanding aorta presses on the nerve leading to the vocal cords.
- Difficulty Swallowing: A feeling of food getting stuck occurs when the aorta presses on the esophagus, which is located directly in front of it.
- Shortness of Breath: Develops as a result of pressure on the trachea.
Emergency: If there is sudden, very severe, “tearing” pain in the back or chest, this is a symptom of aortic dissection (rupture) and requires immediate intervention.
Diagnostic Methods
Diagnosis is usually made incidentally during a chest X-ray or CT scan performed for another reason. For definitive diagnosis:
- Computed Tomography (CT) Angiography: This is the gold standard. The diameter, length, and anatomical structure of the aneurysm are measured in millimeters.
- MR Angiography: Does not involve radiation and is preferred for patients requiring frequent follow-up.
Treatment Options
The treatment decision is made based on the aneurysm’s diameter, growth rate, and the patient’s complaints.
1. Medical Management (Watchful Waiting)
In patients whose diameter has not reached the surgical limit (usually 5.5 cm), blood pressure control and regular CT follow-up are performed. Smoking must be stopped.
2. Endovascular Method (TEVAR)
Today, this is the first choice method for thoracic aortic aneurysms (Thoracic Endovascular Aortic Repair). It does not require open surgery.
- How is it done? A fabric-covered stent (artificial vessel) is advanced from the groin to the area of the aneurysm and placed inside the vessel.
- Advantage: The chest cavity is not opened, blood loss is minimal, and recovery is very fast (1-2 days of hospital stay).
3. Open Surgery
It is preferred for patients whose anatomy is not suitable for TEVAR or in connective tissue diseases such as Marfan syndrome. The chest cavity is opened, the enlarged vessel is cut and removed, and an artificial vessel is sewn in its place.
Risks of Surgery (Stroke Risk)
The most common concern and question patients have regarding thoracic aortic surgery is the risk of paraplegia (paralysis in the legs). Small vessels that supply the spinal cord branch off the thoracic aorta. Affecting these vessels during surgery or stenting can lead to temporary or permanent loss of function.
However, today, with measures such as cerebrospinal fluid drainage (CSF drainage) and controlled elevation of blood pressure, this risk has been reduced to levels as low as 2-3%.
Recovery Process
- After TEVAR: The patient usually gets up the next day and is discharged within 2-3 days. They return to daily life within a week.
- After Open Surgery: 5-7 days of hospital stay and 4-6 weeks of home rest are required.
Frequently Asked Questions (FAQ)
When is thoracic aneurysm surgery necessary?
Intervention is generally required when the aortic diameter reaches 5.5 cm or more, or when it grows more than 0.5 cm per year. In genetic conditions like Marfan syndrome, the limit may be 4.5 – 5.0 cm.
Can TEVAR (Endovascular method) be applied to everyone?
No. For TEVAR to be applicable, there must be healthy vessel segments (landing zones) at the beginning and end of the aneurysm where the stent can anchor. Also, the vessel structure should not be excessively tortuous. Suitability is determined by CT angiography.
Does an aneurysm shrink on its own?
No, an enlarged aortic vessel does not shrink on its own. Medications can only slow down the growth rate and prevent rupture. The definitive solution is mechanical repair (stent or surgery).
Is the risk of paralysis high?
This risk, which used to be high, has significantly decreased thanks to modern techniques and the TEVAR method. In experienced centers, this rate is below 5%.