
If the vessel diameter reaches critical limits, it poses life-threatening risks such as internal tearing of the vessel wall (Aortic Dissection) or complete rupture. However, with early diagnosis and regular follow-up, these risks can be managed, and complete treatment can be provided with surgical intervention when necessary.
Where is the Ascending Aorta and Why Does It Enlarge?
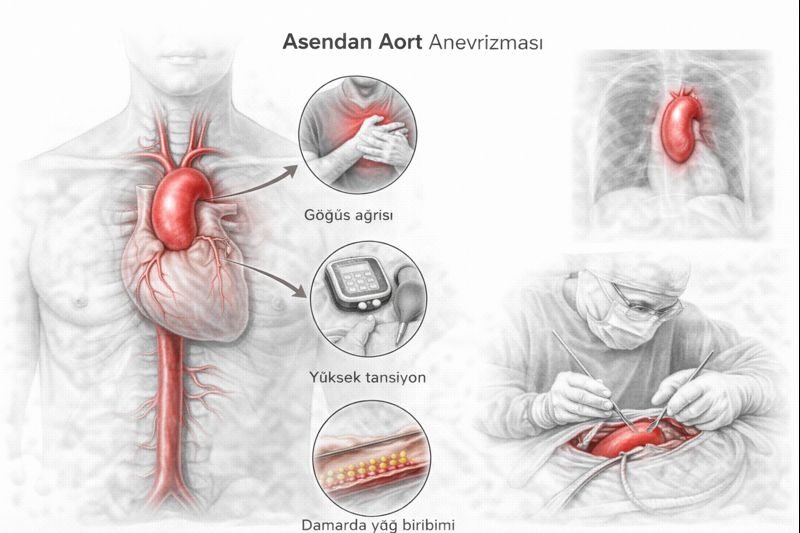
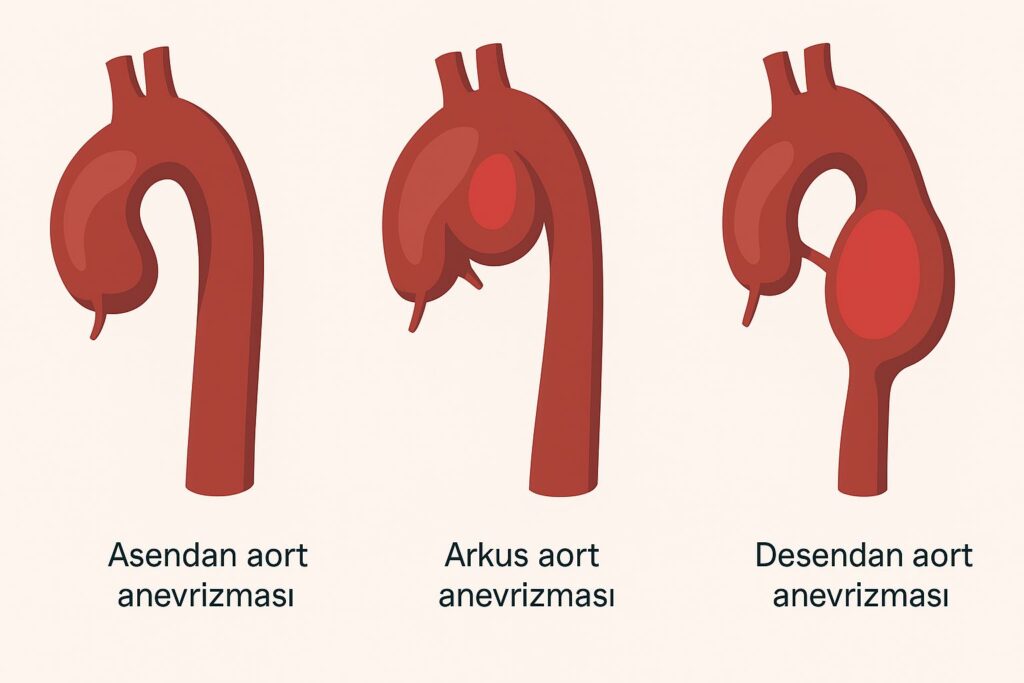
The aorta emerges from the left ventricle of the heart and descends, taking on a cane shape. The first 5-6 cm section where it exits the heart is called the `“Ascending Aorta”`.
This region is the first to be exposed to the high pressure (jet flow) created by the blood pumped with each heartbeat. Over time, the elastic fibers in the middle layer of the vessel wall deteriorate (degeneration), reducing the vessel’s resistance to pressure and causing it to expand outwards. Normally, the diameter should be 2.5 – 3.5 cm; an aneurysm is diagnosed when it reaches 4 cm or more.
Causes and Risk Factors
There is no single cause for ascending aortic aneurysm; it is usually a combination of genetic predisposition and environmental factors.
- Hypertension (High Blood Pressure): Uncontrolled blood pressure continuously hammers the vessel wall, causing it to weaken.
- Bicuspid Aortic Valve: This is a congenital condition where the aortic valve, which should normally have 3 leaflets, has only 2. In these patients, the aortic wall tissue is genetically weaker, and the turbulent blood flow significantly increases the risk of aneurysm.
- Connective Tissue Diseases: Genetic diseases such as Marfan Syndrome, Ehlers-Danlos, and Loeys-Dietz Syndrome impair collagen and elastin in the vessel structure.
- Atherosclerosis (Hardening of the Arteries): This is the accumulation of plaque in the vessel wall due to smoking, high cholesterol, and advanced age.
- Family History: The risk increases in individuals with a family history of aneurysm or sudden death.
The Body’s Signals: Symptoms
Unfortunately, most aneurysms do not cause any symptoms and are usually found incidentally during a CT scan or echocardiography performed for another reason. However, when the diameter becomes very large, it can press on surrounding tissues, leading to the following complaints:
- A deep, dull chest pain or pressure sensation.
- Hoarseness if it presses on the nerve going to the vocal cords.
- Shortness of breath or cough if it presses on the windpipe.
- Difficulty swallowing if it presses on the esophagus.
IMPORTANT: If there is sudden, severe, “tearing-like” pain in the chest radiating to the back, this is a symptom of Aortic Dissection (rupture), and 112 should be called immediately.
The Greatest Fear: Aortic Dissection
The most feared complication of an aneurysm is dissection. The expanding vessel wall thins, and its inner layer tears. Blood enters between the vessel layers, separating the vessel along its length. This can impair organ perfusion and lead to fatal hemorrhages. Aneurysm treatment is performed precisely to prevent this scenario.
Diagnostic Methods
- Echocardiography (ECHO): This is the first-line screening test. The aortic root and valve structure are visualized.
- Computed Tomography (CT) Angiography: This is the gold standard for diagnosis. The aortic diameter is measured in millimeters, and its size and extent are clarified. The surgical plan is made accordingly.
- MR Angiography: It does not involve radiation and is preferred for young patients requiring frequent follow-up or those with kidney failure.
Treatment Options
Not every aneurysm is operated on. The treatment plan is like a “balancing scale”; the risk of surgery is compared to the risk of vessel rupture.
1. Medical Follow-up and Lifestyle
In patients whose diameter has not reached the surgical limit (e.g., < 4.5 cm):
- Blood Pressure Control: It is essential to keep blood pressure below 120/80 mmHg (Beta-blocker medications are usually prescribed).
- Regular Imaging: Growth rate is monitored every 6 or 12 months with CT or ECHO.
- Avoid heavy lifting (like bodybuilding) and sports that require straining.
2. When is Surgery Decided?
According to international guidelines, surgical limits are as follows:
| Patient Group | Aortic Diameter Limit |
|---|---|
| Standard Patients | 5.5 cm and above |
| Marfan Syndrome / Connective Tissue Disease | 4.5 – 5.0 cm |
| Bicuspid Aortic Valve Patients | 5.0 – 5.5 cm |
| Patients Undergoing Other Heart Surgery | 4.5 cm (Performed simultaneously) |
Additionally, regardless of the diameter, if there is rapid growth of more than 0.5 cm per year, a decision for surgery is made.
3. Surgical Techniques (Bentall and Graft)
Performed via open-heart surgery by opening the breastbone.
- Tube Graft Replacement: If the aortic valve is healthy, it is preserved; only the enlarged vessel section is removed and replaced with a synthetic artificial vessel (Dacron graft).
- Bentall Operation: If the aortic valve is also damaged or the aneurysm is very close to the valve, both the vessel and the valve are replaced as a single unit (valved conduit).
- David Operation: If the valve leaflets are healthy, the valve is preserved, and only the vessel is replaced. This is technically more challenging but advantageous for the patient.
Post-Surgery Recovery
After successful surgery, patients are usually discharged after 1 day in intensive care and 4-5 days of ward follow-up. Full recovery and bone healing take 6-8 weeks. Post-surgery, blood pressure control remains important for life.
Frequently Asked Questions (FAQ)
Can an aortic aneurysm rupture?
Yes, when the aneurysm diameter reaches a certain size (usually over 6 cm), wall tension increases, and there is a risk of spontaneous rupture. Therefore, having elective (planned) surgery before reaching the critical limit is life-saving.
I have an aneurysm, can I exercise?
Light to moderate intensity walks and isotonic exercises like swimming are beneficial. However, sports that cause sudden blood pressure spikes and require straining (isometric), such as weightlifting (bodybuilding), push-ups, and pull-ups, are prohibited.
Is the surgery very risky?
Surgeries performed in emergency conditions (when the vessel has ruptured) carry a high risk. However, in planned surgeries performed before the vessel ruptures, the risk is around 1-3%, and the success rate is quite high.
Can this disease be passed on to my children?
If your aneurysm is due to a genetically inherited condition such as Marfan syndrome or bicuspid aortic valve, there is a possibility that your children may also have it. It is recommended that your first-degree relatives also undergo ECHO screening.