
Coronary Bypass Surgery or Stent? How is the decision made?
Key Differences: What are Stent and Bypass?
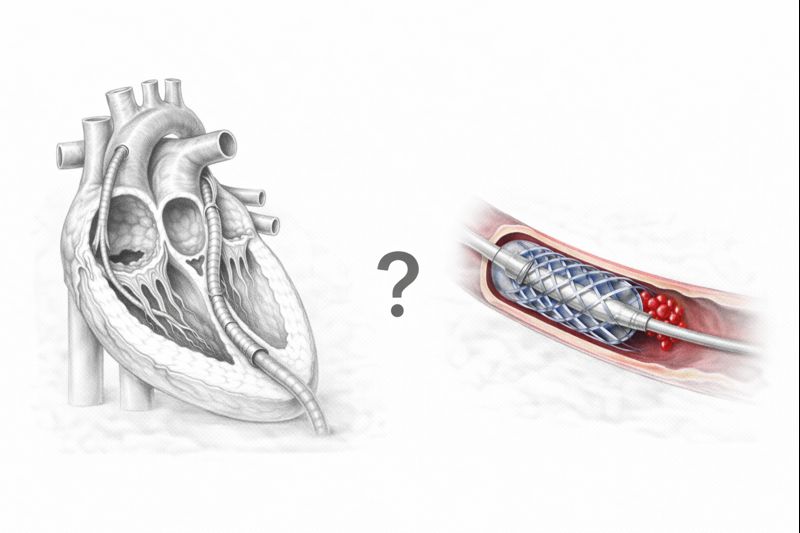
Although both methods aim to improve the heart’s blood supply, their mechanisms and application methods are completely different.
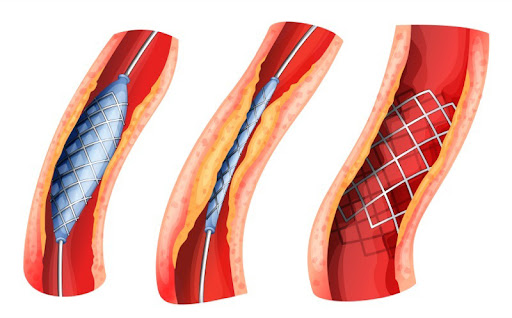
Percutaneous Coronary Intervention (Stent): Popularly known as “ballooning” or “cage placement.” It is a procedure performed by entering through the artery in the groin or wrist, typically not requiring surgical incision. In the angio laboratory, a thin wire reaches the narrowed area, the narrowing is first widened with a balloon, and then a metal cage (stent) is placed to prevent the vessel from collapsing again.
Coronary Artery Bypass Grafting (CABG): Instead of opening the blockage itself, a new vessel pathway (bridge) is created to bypass the blocked area. Healthy vessels taken from another part of the body (from inside the chest, arm, or leg) are sewn beyond the blockage. Thus, blood reaches the heart through the new pathway without using the blocked one.
[Image of coronary artery bypass grafting illustration]
Stent Treatment: Advantages and Limitations
With technological advancements, stents are life-saving, especially in acute situations.
- Speed and Comfort: The chest is not opened, and general anesthesia is not required. The patient is usually awake during the procedure.
- Short Hospital Stay: If no complications arise, the patient can be discharged after 24 hours and return to work within a few days.
- Drug-Eluting Stents: In older metal stents, the risk of re-narrowing of the vessel was higher. Today’s drug-coated stents reduce this risk to 5-10% by preventing cell proliferation.
Limitations: If the vessel structure is very calcified, tortuous, or the narrowing is very long, stent placement can be technically difficult or the success rate may decrease. Furthermore, a stent does not eliminate the plaque within the vessel; it merely presses it against the wall.
Bypass Surgery: Situations Where It Is the Gold Standard
Bypass, being “open-heart surgery,” can be intimidating for patients, but in terms of long-term results, it is unrivaled, especially in complex cases.
- Complete Revascularization: In bypass surgery, the surgeon bypasses the blocked vessel, regardless of how calcified it is, and sews the vessel to a clean area. This ensures a much more guaranteed blood flow.
- Long-Lasting Solution: Especially when the internal mammary artery (LIMA) is used, the patency rate of this vessel for 10-20 years is over 90%.
- Protection Against Heart Attack: Even if the main vessel in the bypassed area becomes completely blocked in the future, the risk of heart attack is very low as long as the bypass graft is functioning.
How is the Decision Made? The “Heart Team” Approach
In modern medicine, this decision is not left to the discretion of a single doctor. The “Heart Team,” consisting of Cardiologists and Cardiovascular Surgeons, collectively evaluates the patient’s angiographic images and clinical condition.
The most important factors influencing the decision are:
- Extent of Vessel Involvement (SYNTAX Score): If there are short and simple narrowings in only one or two vessels, Stent is preferred. However, if there is three-vessel disease, narrowings affecting bifurcation areas, or widespread calcification, the score will be high, and Bypass is recommended.
- Left Main Coronary Artery Disease: If there is narrowing in the main artery supplying 70% of the heart, surgery is generally considered safer and more long-lasting.
- Heart Function: In patients with reduced heart pumping strength (EF), bypass surgery is more successful in preserving heart function in the long term.
Critical Choice for Diabetic Patients
Diabetic patients constitute a special group. Diabetes diffusely damages the vessel structure; meaning there can be sequential narrowings along the vessel like a string of pearls.
Scientific studies (e.g., the FREEDOM trial) have clearly shown that bypass surgery prolongs life expectancy and reduces the risk of heart attack more significantly than stent treatment in diabetic patients with multi-vessel disease. Stents tend to re-occlude more frequently in diabetic patients. Therefore, for diabetic patients, the needle often points more towards surgery.
Comparison of Recovery Processes
In terms of patient comfort, stents are clearly ahead, but “recovery” is not just wound healing.
- After Stent: Physical recovery takes 1-2 days. However, the patient must strictly adhere to antiplatelet medications (dual therapy). Stent placement does not mean the disease is over; if lifestyle changes are not made, narrowing may occur elsewhere.
- After Bypass: The average hospital stay is 5-7 days. To allow the breastbone to heal, one must lie on their back for 4-6 weeks and avoid heavy lifting. Full recovery and increased exercise capacity can take 2-3 months. However, once recovery is complete, the patient generally feels more unrestricted in terms of exercise capacity than a patient with a stent.
Summary: Frequently Asked Questions (FAQs)
What is the main difference between coronary bypass and stent?
Is a stent more risky or bypass surgery?
Can a stented vessel become blocked again?
How long does a patient live after bypass surgery?
More About the Difficult Decision
Stent or bypass? Which is better for diabetic patients? You can review our special page prepared to answer the 25 most frequently asked questions about the decision-making process, risks, and long-term results.
Life After Treatment and Medication Use
Whichever method is chosen, the underlying disease of “arteriosclerosis” continues. Therefore, the post-treatment process is at least as important as the procedure itself.
- Medications: Stent patients must use two different antiplatelet medications for a certain period (discontinuation can lead to clot formation within the stent). For bypass patients, a single antiplatelet (aspirin, etc.) is usually sufficient.
- Lifestyle: Smoking must be absolutely quit. A Mediterranean diet, regular walking, and control of blood pressure and cholesterol should be maintained.
Conclusion: Joint Decision
The best treatment is one that aligns the patient’s medical realities with their social expectations. If your doctor tells you, “Either a stent or surgery is possible,” do not hesitate to ask about the risks and 10-year expectations of both methods. Remember; the goal is not just to save today, but to live a long and healthy life.